43
| 3 | 2012
Klinisk Biokemi i Norden
angiotensin II receptor blockers this was suggested by
23–50% (
depending on the country).
For Article III, the response rate was 60%, and 210
patients were included. The median creatinine values
were 95 and 124 µmol/l for female and male patients;
the corresponding eGFR values were 52 and 51 ml/
min/1.73m2. Only 27% of patients were assessed to
have CKD stage 3. Two-thirds had a urine dip strip
(59%)
and/or a urinary albumin (42%) measurement,
and 20% were diagnosed with albuminuria (including
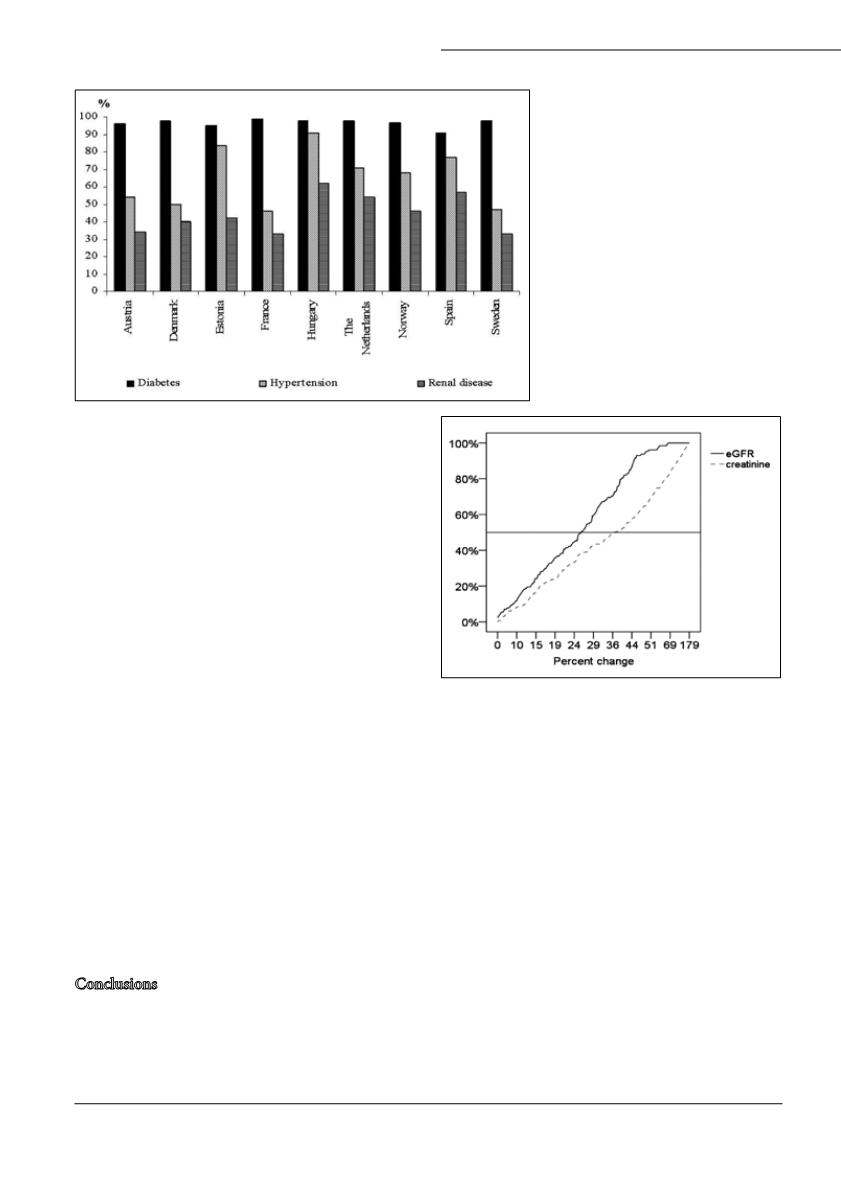
both micro- and macroalbuminuria). The changes in
creatinine and eGFR values that GPs suggested indi-
cative of referral to nephrology or internal medicine is
shown in figure 2. Albuminuria did not influence the
follow-up strategy.
For Article IV, 52 (52%) laboratory specialists respon-
ded. Based on guideline recommendations, less than
30%
would suggest an optimal test panel for evaluating
renal function in the two primary-care patients. For
creatinine and eGFR, the median changes considered to
signal improvement or deterioration in renal function
(
creatinine, 14% and 14%, respectively; eGFR, 18% and
13%,
respectively) were similar to what could be calcula-
ted using information on analytical and within-subject
variations from the literature. The albumin:creatinine
ratio varied (median values: 50% for improvement and
67%
for deterioration).
Conclusions
Guidelines for diagnosing microalbuminuria are only
partially followed by general practitioners, and should
be made more practicable, addressing issues such as
type of samples, measurement units and repeat tests.
Intensified drug treatment, and especially increased
use of ACEIs and ARBs, was recommended to diabetic
patients when microalbuminuria was present. CKD
stage 3 patients were insufficiently examined for albu-
minuria and seemingly referred to hospital care only
after the eGFR declined more than recommended in
guidelines. Renal parameters are interpreted differently
by laboratory specialists, and this could result in dif-
ferent advice being offered to clinicians, which again
may affect patient care. Both in general practice and
laboratory medicine more and coordinated information
is necessary upon implementing changes in commonly
used laboratory tests.
Kristin Moberg Aakre disputerte 12. oktober 2011 for
PhD.-graden ved Universitetet i Bergen. Avhandlingen
i sin helhet er tilgjengelig elektronisk fra Bergen Open
Research Archive
2011.
Figure 1. Reasons for requesting urine albu-
min in nine different European countries.
Figure 2. Cumulative percentage changes
in creatinine and eGFR values suggested
by GPs to indicate referral of CKD stage
3
patients to a specialist in nephrology
or internal medicine. The horizontal line
denotes the median value.


