42
| 3 | 2012
Klinisk Biokemi i Norden
Doktorgradsavhandling:
Bruk og tolkning av urin albumin og estimert
GFR i allmennpraksis
Kristin Moberg Aakre
Institutt for Samfunnsmedisinske fag, Universitetet i Bergen
kristin.moberg.aakre@helse-bergen.no
The daily work of physicians includes a constant flow
of information. In this context, it is understandable that
laboratories can experience difficulties informing phy-
sicians about the introduction of new laboratory tests
or about changes in the use of well-known tests. The
data presented here was collected to focus on one main
aspect in the tasks of modern laboratories: the respon-
sibility to help physicians to choose the best available
test procedures, and to get the most out of the informa-
tion provided by the test results, thereby facilitating the
correct diagnosis and follow-up of patients. Chronic
kidney disease (CKD) was chosen to explore the topic
since laboratory tests are crucial for the diagnosis and
the test procedures and interpretation of “old tests” (i.e.
serum creatinine and urine protein) has changed during
recent years. At present CKD may be diagnosed based
on an estimated glomerular filtration rate (eGFR) that is
calculated from creatinine data, and the prognosis may
be predicted based on urinary albumin excretion. Our
work elucidated how urinary albumin and eGFR are
used and interpreted in the primary health-care setting.
Another focus was to assess how the clinical chemistry
laboratories that usually offer these tests interpret the
test results.
Four articles were included in the thesis and all data
were collected with the aid of a questionnaire. For Artic-
les I and II, 10,000 general practitioners in 11 countries
received a case-history-based questionnaire depicting a
male type 2 diabetes patient. For Article III, 386 Norwe-
gian physicians received a questionnaire asking about
1
of their patients (selected from 2 different hospital
laboratory databases) who had been diagnosed with
CKD stage 3, based on eGFR results. For Article IV, 100
laboratory specialists in Norway and the Netherlands
received a questionnaire regarding 2 case histories from
primary health care (hypertensive and diabetic patients
with laboratory results signalling possible renal disease)
and 1 from a hospital setting.
The studies described in Articles I and II included
2078
general practitioners from 9 European countries.
Almost all of the general practitioners recommended
annual microalbuminuria testing in diabetic patients,
whilst a lower frequency of testing was suggested for
patients with hypertension or possible CKD (figure 1).
Of the 2078 general practitioners, 62% requested the
recommended repeated test to confirm the diagnosis of
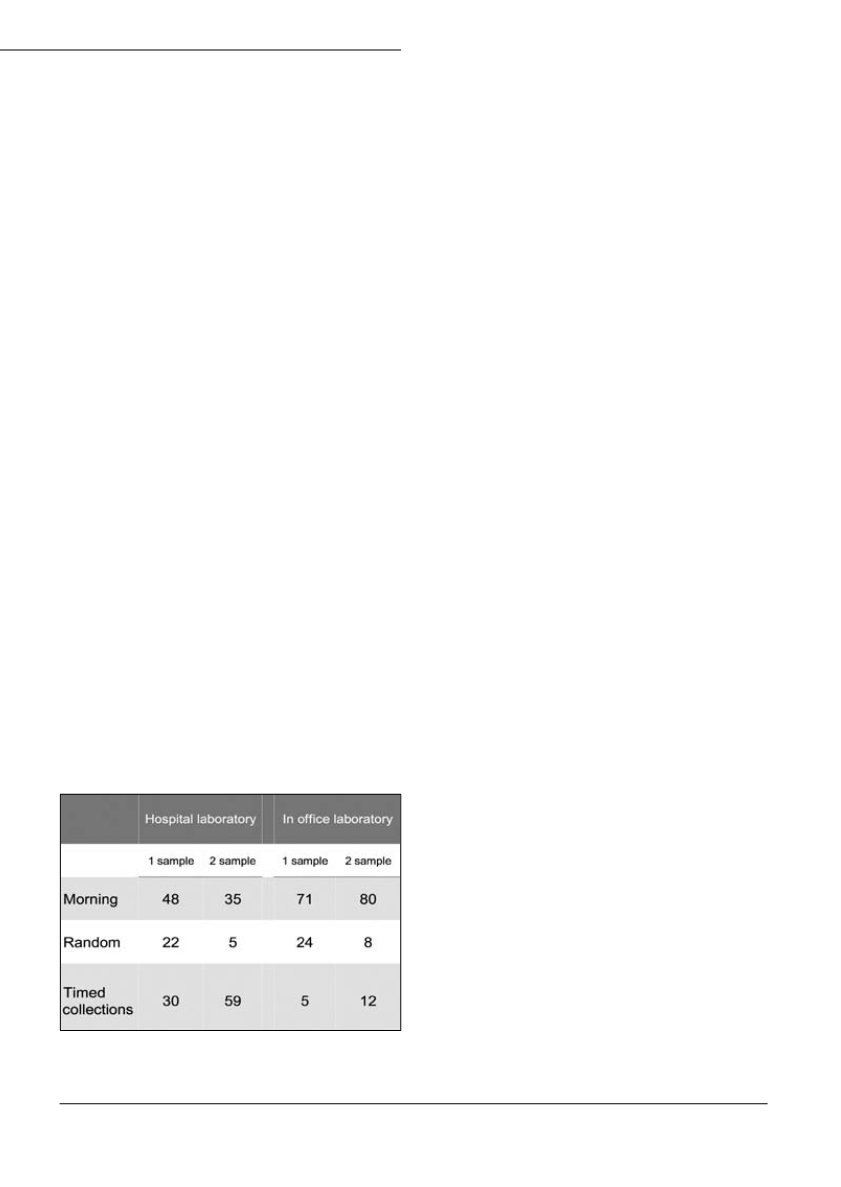
albuminuria if the first test was positive. Table 1 show
that the recommended morning urine sample prevailed
for first-time office-based testing, whilst cumbersome
timed collections were used to a larger extent for hos-
pital-based repeat testing. The median values for the
critical difference in albumin concentration was 33%
i.e. lower then what may be calculated based on analy-
tical and within-subject biological variance (100-200%).
Almost all general practitioners would supplement the
patient’s drug treatment if microalbuminuria develo-
ped; for angiotensin-converting enzyme inhibitors or
Table 1. Percentages of GPs requesting different sampling met-
hods stratified according to type of laboratory used.


