23
| 1 | 2012
Klinisk Biokemi i Norden
(
Fortsætter side 24)
first shown to support a DI diagnosis in patients with
complete central DI following transsphenoidal sur-
gery. Copeptin concentrations below 4.5 pmol/L after
insulin-induced hypoglycemia separated all patients
compared to normal controls (4). This is, however, far
from the clinical reality where the majority of patients
will present with incomplete forms of DI or primary
polydipsia. Recently, copeptin was tested in a more
everyday-like situation and the results were compared
to the standard diagnostic procedure in patients with
partial central DI, complete central DI, nephrogenic
DI, and primary polydipsia. Copeptin measurements
during the water deprivation test were shown to have
superior diagnostic power compared to all other ana-
lyses including vasopressin measurements (5). Due to
overlap between controls and patients with different
forms of polydipsia, the actual copeptin concentrations
during the water deprivation test showed limited diag-
Copeptin measurement in plasma
An automated platform has been introduced for
routine copeptin plasma measurement. Copeptin is
measured by a sandwich assay utilizing antibodies
directed against distinct epitopes in the copeptin pri-
mary sequence (provasopressin 113-128 and 130-145,
respectively). The method was validated and published
in 2006, where the marked in vitro stability of copep-
tin seems to provide a promising tool for evaluating
the vasopressin response in human health and disease
(3).
A more sensitive assay has now been launched
(
in 2011) that allows for copeptin measurement even
in the low picomolar range (1 pmol/L). Notably, this
is required for clinical measurement, where low or
no vasopressin production is suspected. Copeptin
measurement, however, is still largely defined by one
company and their automated platform, which makes
comparison to other methodologies impossible. Thus,
all copeptin plasma measurements in new clinical stu-
dies refer to this specific methodology. In the following
sections, we have included clinical scenarios, where
copeptin measurement may provide clinically relevant
information beyond existing markers.
Copeptin and diabetes insipidus
Diabetes insipidus (DI) is suspected when patients
have excessive fluid intake (polydipsia) and produce
large volumes of dilute urine, usually over 3 L/day. The
pathogenesis behind the polydipsia-polyuria syndrome
is either an insufficient vasopressin secretion (central
DI), insufficient vasopressin response in the kidneys
(
nephrogenic DI) or excessive water intake caused by
other reasons such as defects in thirst perception or
psychogenic reasons (primary polydipsia). The final
diagnosis relies on laborious tests where patients are
admitted and asked to refrain from drinking during
a day usually followed by a desmopressin challenge,
while analyses for urine osmolarity, plasma osmola-
rity, and plasma sodium are performed. These tests,
however, have limited diagnostic accuracy because
the most common form of DI is due to a reduced
rather than a total loss of either vasopressin produc-
tion or response in the kidneys. In addition, most
patients with polydipsia have primary polydipsia.
To overcome this problem, it is recommended to
quantitate vasopressin during the water deprivation
test. Due to the methodological problems mentioned
in the introduction, this has not been included as
a diagnostic standard. Copeptin measurement was
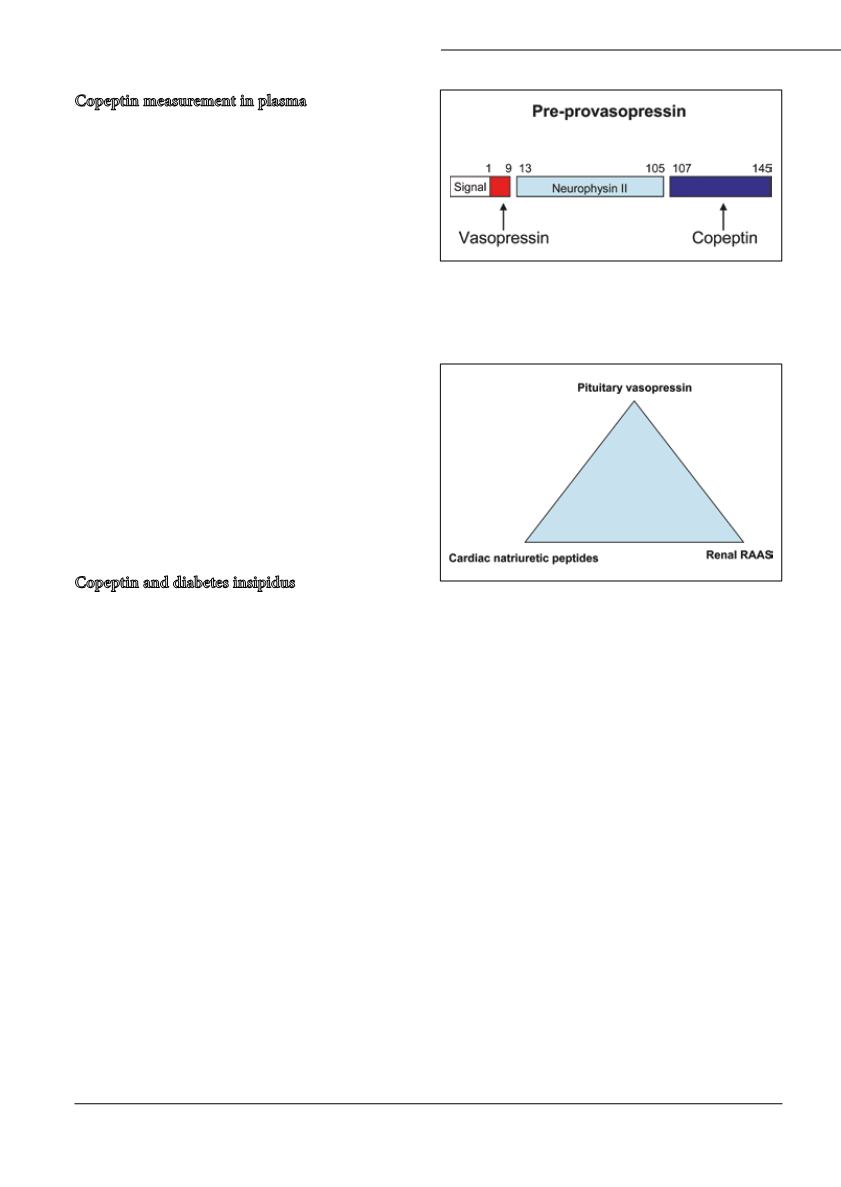
Figur 2:
Schematic presentation of the human vasopressin
precursor. Copeptin constitutes the C-terminal fragment and
vasopressin the N-terminal peptide from the prostructure.
Figur 3:
Triangle of peptide hormones involved in water
homeostasis. Note that all hormones are key players in cardio-
vascular pathophysiology and treatment.


