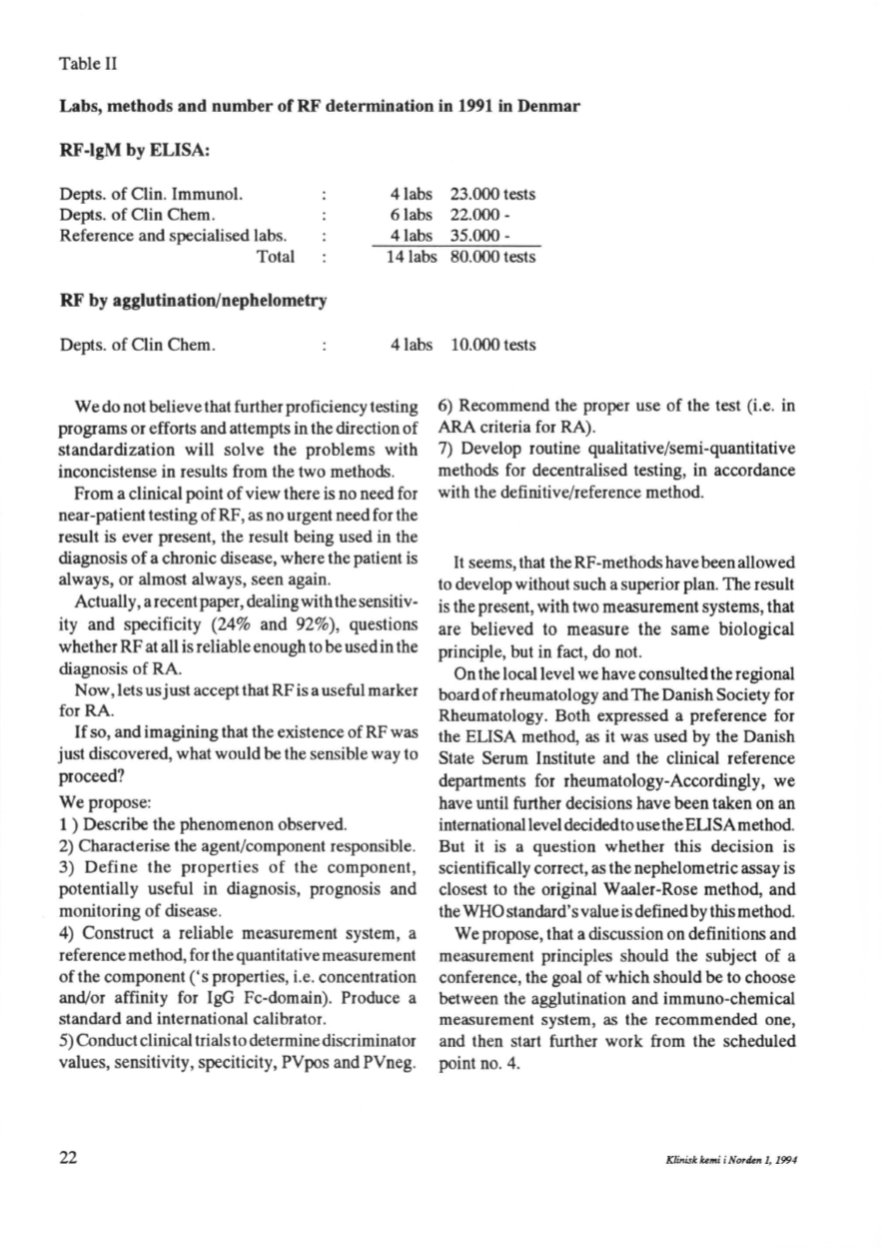
Table Il
Labs, methods and nomber of RF determination in 1991 in Denmar
RF
-lgM
by ELISA:
Depts. of Clin. Immunol.
Depts. of Clin Chem.
Reference and specialised labs.
4labs 23.000 tests
6labs 22.000-
4labs 35.000 -
Total
14labs 80.000 tests
RF by agglutination/nephelometry
Depts. of Clin Chem.
4labs 10.000 tests
We do not believe that further proficiency testing
programs or efforts and attempts in the direction of
standardization will solve the problems with
inconcistense in results from the two methods.
From a clinical point of view there is no need for
near-patient testing of RF, as no urgent need for the
result is ever present, the result being used in the
diagnosis of a chronic disease, where the patient is
always, or almost always, seen again.
Actually, a recent paper, dealingwith the sensitiv–
ity and specificity (24% and 92%), questions
whetherRFat all is reliable enough to be used in the
diagnosis of RA
Now, lets usjust accept that RF is a useful marker
for RA.
If
so, and imagining that the existence of RF was
just discovered, what would be the sensible way to
proceed?
Wepropose:
l )
Describe the phenomenon observed.
2) Characterise the agent/component responsible.
3) Define the properties of the component,
potentially useful in diagnosis, prognosis and
monitoring of disease.
4) Construct a reliable measurement system, a
referencemethod, for the quantitative measurement
of the component ('s properties, i.e. concentration
and/or affinity for IgG Fc-domain). Produce a
standard and international calibrator.
5) Conduct clinical trials to determine discriminator
values, sensitivity, speciticity, PVpos and PVneg.
22
6) Recommend the proper use of the test (i.e. in
ARA criteria for RA).
7) Develop routine qualitative/semi-quantitative
methods for decentralised testing, in accordance
with the definitive/reference method.
lt
seems, that theRF-methodshavebeenallowed
to develop without such a superior plan. The result
is the present, with two measurement systems, that
are believed to measure the same biological
principle, but in fact, do not.
On the locallevel we have consulted the regional
board of rheumatology and The Danish Society for
Rheumatology. Both expressed a preference for
the ELISA method, as it was used by the Danish
State Serum Institute and the clinical reference
departments for rheumatology-Accordingly, we
have until further decisions have been taken on an
internationallevel decidedto usetheELISAmethod.
But it is a question whether this decision is
scientifically correct, as the nephelometric assay is
dosest to the original Waaler-Rose method, and
theWHO standard's value is definedby thismethod.
We propose, that a discussion on definitions and
measurement principles should the subject of a
conference, the goal of which should be to choose
between the agglutination and immuno-chemical
measurement system, as the recommended one,
and then start further work from the scheduled
point no. 4.
Klinisk Umi
i
NortUn 1, 1994


