Klinisk Biokemi i Norden · 3 2019
| 13
lity. Whereas overt Se deficiency in humans is rare,
there are indications that suboptimal Se supply may
affect aspects of human health, and thus contribute
to cardiovascular disease, cancer, defective immune
response, and neurodevelopmental and neurodegene-
rative conditions (2). The expression of selenoproteins
is generally dependent on the supply of the trace ele-
ment through food. The content in food varies greatly
between different geographical areas, dependent on the
soil content of selenium. Cereals, meat, fish, and dairy
products are main sources of selenium. European soils
are low in selenium and consequently, intake levels of
selenium are generally low and in many cases below
recommended intakes (4,5), whereas they are consi-
derably higher in North America, where many of the
studies investigating beneficial effects of selenium sup-
plementation have been conducted (Figure 1). Higher
intake levels in Finland are due to selenium addition
to fertilisers and in Norway to import of wheat. The
intake level in segments of the populations in each
country may vary largely.
Up till now relatively little attention has been paid
to selenium intake and status in clinical medicine,
even if there is accumulating evidence that selenium
status might be important in various diseases. Sele-
nium analyses in blood or serum/plasma are available
in some larger medical laboratories. In European and
Scandinavian laboratories, the lower end reference
limits reflect the selenium status in the respective
populations and are often far below values compatible
with an adequate intake. In this review, we provide
recent insights in the biochemical role of selenium,
and an update on possible role of suboptimal intake in
the pathogenesis of important diseases in our society.
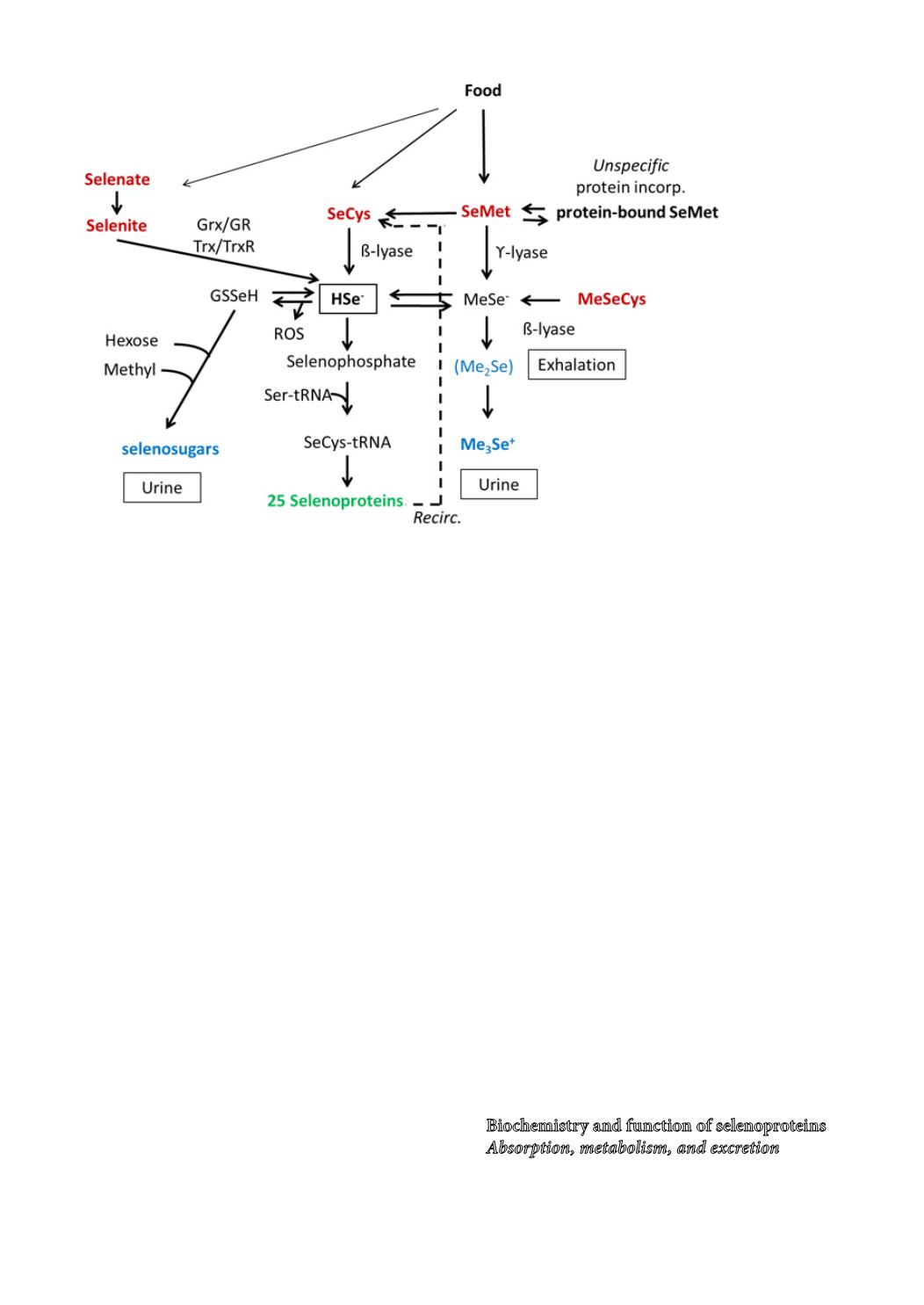
Biochemistry and function of selenoproteins
Absorption, metabolism, and excretion
Water-soluble selenomethionine, the major selenium
Figure 2.
Metabolism of selenium and
synthesis of selenoproteins.
Dietary selenium (red) are selenomethionine and selenocysteine from proteins, iorganic salts and low molecular organic
selenium. The reduction of selenite requires glutathione (GSH), glutarexin (Grx), glutathione reductase (GSR) and/ or thiore-
doxin (Trx)/ thioredoxin reductase (TrxR). Selenium is specifically incorporated into selenoproteins (green) via selenide and
synthesis of selenophosphate by the selenoprotein selenophosphate synthase 2. SeCys from selenoproteins is degraded and
reused. Selenomethionine (SeMet) can split off methylselenide or be converted to selenocysteine (SeCys) via the cystathion
pathway. SeMet may also enter the “methionine pool” and unspecifically replace its sulfur analogue in proteins. Among
excretory metabolites (blue) are selenosugars and at high doses trimethyl selenonium ion (Me
3
Se
+
). Intoxications may lead
to excess dimethylselenide (Me
2
Se) that may cause a garlic breath. Surplus of selenide may redox cycle and produce reactive
oxygen species (ROS).


